

A Blood Test Claims 100% Accuracy in Screening for Cancers
In other breaking news: A sucker is born every minute.

Frequently in medicine, a study makes a modest or nuanced assertion that is then amplified to the nth degree by the media in attempt to draw attention. The headline sent to me by a friend this morning, however, is impossible to overstate: a firm based in India and Singapore, Tzar Labs, is claiming to have developed a blood test that can detect and describe every form of cancer, even before a tumor has started to form, with perfect accuracy. I exaggerate not a bit. Most major news outlets opted to pass on reporting this piece of news. The New York Post, however, took it, and ran:

It’s the sort of read that gets would-be investors checking their accounts for liquidity, and consumers asking how they can sign up. I mean, how good is this HrC test? It’s perfect!
My eyebrows knitted upon reading this claim. Nothing in medicine is perfect! The last time I saw something that claimed to be 100% effective, it was that Argentinian study on ivermectin showing that it prevented 100% of Covid-19 cases in health care workers. The catch? The study apparently never actually took place.
Fortunately, we do have the published research used to support these claims about the HrC test. In the journal, Stem Cells Reviews and Reports, the paper describes testing for a type of cancer stem cell expressing a marker, OCT-4A, with remarkable results. After setting parameters by testing on 120 cancer patients, they applied these cut-offs to 1000 patients, half of whom were known to have cancer; the other half, presumed to be cancer-free. Everyone without cancer was under their cut-off numerical value of 10; everyone with cancer was above. Every rise of 10 points meant the stage of disease went up one notch; in other words, stage one cancers all scored between 10-20, stage two between 20-30, and so on. Talk about neat findings!
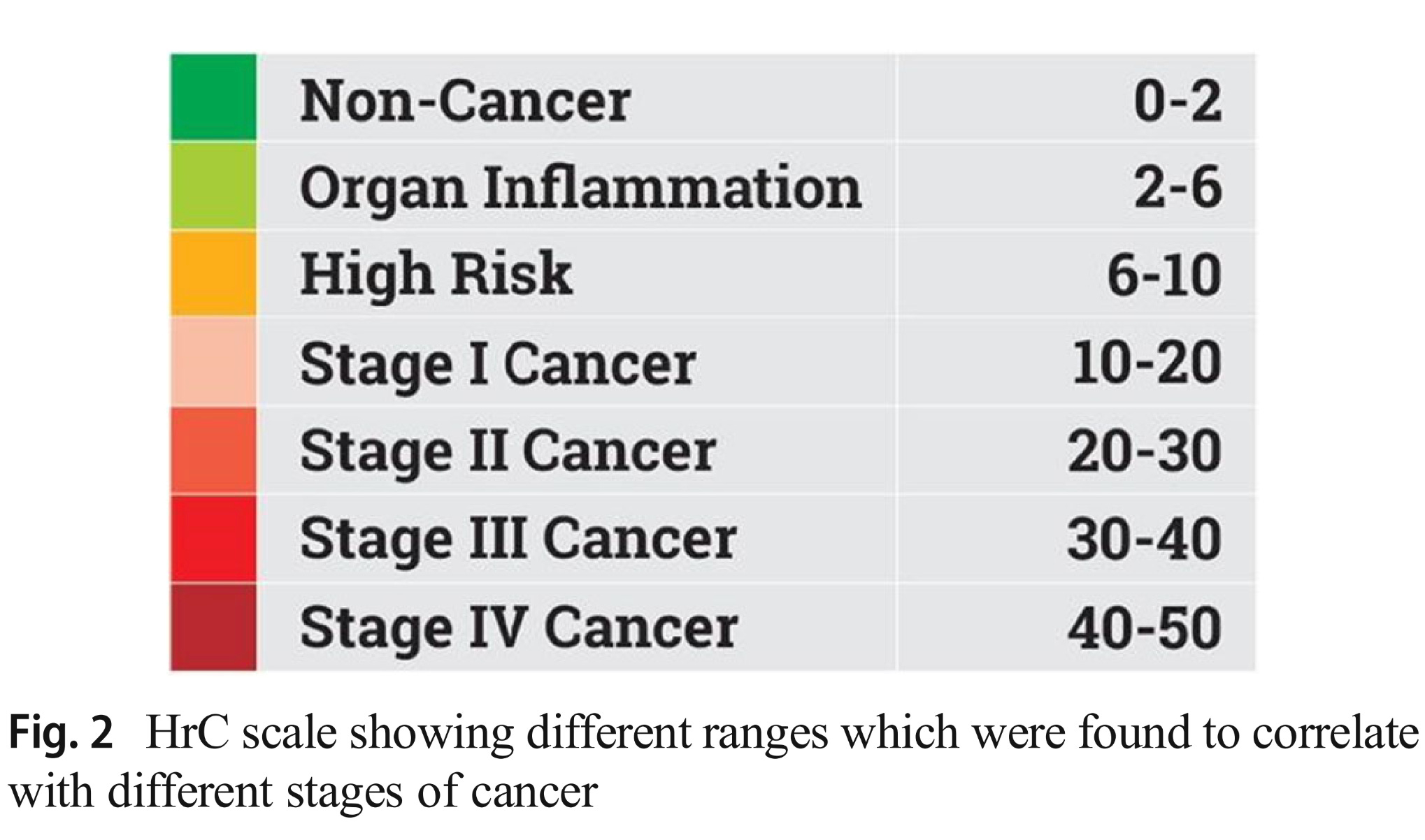
While it’s hard to believe the authors really intended to claim that every single test nailed the stage, see for yourself:

From the text, that sure seems to be the implication, too.

Best of all, though, the miss rate was zero. Zero. If you did not have cancer, your test was negative (except for a few in the high-risk category, who, of course, were followed and found to actually have cancer!); if you did have a known cancer, your test was positive. Every single time. Perfect. I am not making this up!

It’s really so jaw-droppingly absurd that I felt compelled to write the lead author, Dr. Deepa Bhartiya, who promised a response later today; I will update if she responds (please reference Update below article). Perhaps some of you, less jaded than I, see these numbers and feel a burgeoning excitement. I just see bullshit. Allow me to explain.
While I am not an oncologist, and a genuine oncologist would certainly have a more educated take on the theory behind the HrC test, I don’t need to be an expert to know these reports are unlikely to pan out. For one, the biology behind this test — as admitted by the authors of their advertisement-like recent publication in the peer-reviewed (!) journal, Stem Cells — is still a matter of controversy. There is some general agreement that stem cells play a central role in the creation of tumors. Less so, though, that the entity they describe as Very Small Embryonic-Like stem cells (VSELs) in particular do so; and that the marker they test for, OCT-4A, is a reliable indicator of the presence of VSELs bound to become cancer. For instance, studies of ovarian cancer and bladder cancer did find a much higher incidence of OCT-4A in cancer cells than in normal ovarian and bladder tissue cells — but a fair proportion of healthy cells still expressed OCT-4A, at least in modest amounts. While it’s plausible, if a bit of a reach, to believe that VSELs are the essential mediator of cancer, and that OCT-4A is a reliable marker for cancer-prone VSELs, and one could consistently find these in the bloodstream with a single standard blood draw of two teaspoons (10ml) — it’s sure not likely, and it stretches the imagination that levels would so consistently line up neatly with the amount of tumor present for any type of cancer.
The way most evidence-loving scientists look at new concepts is pretty simple: set the probability that something could be true based on existing knowledge, assess the quality and nature of the data in support of the claim, and then adjust one’s prior assumptions. If someone tells you they can give you a shot in your left arm and you’ll live to be 150, your prior probability of this being true would be <0.0001%, since no human has ever lived so long; it would take some remarkable evidence to move the needle enough to take the shot.
HrC is more plausible, true; but if you asked me for odds that a blood test, brought to market by a firm headed by venture capitalists, promoted by Deepak Chopra, banking on an uncertain biological premise, would achieve perfect accuracy in detecting 25 types of cancer… I would have to say <0.1%. Does a single retrospective study, with the authors almost entirely on the company payroll, move that needle enough to be excited? No.
I suspect if a skeptical soul had access to the raw data from that 2021 study, they would find some issues. Lacking that access, we’re left to wonder whether deliberate fraud was behind the stunning numbers, or flawed data collection, or a profound mistake in the analysis. It’s frustrating that a peer-reviewed journal would publish work that can literally be considered the most important research of the century if it were confirmed, without raising these questions publicly.
Now, what would be plausible is if the HrC test, or another similar blood test, ultimately will end up a useful part of our cancer screening process. Prior to this bombshell from Mumbai, I had been planning to write about the Mayo Clinic’s proprietary Grail test, the Galleri, probably the best known player in this field. Unlike HrC, which looks for markers of malignant VSELs, Galleri samples for tumor DNA fragments. It’s not terribly sensitive, missing over 80% of stage I tumors (improving to 10% at stage IV, when it’s not a very useful “screen”), but it’s quite specific, claiming to only report one false positive every 200 tests. On paper, it’s not a bad way to spend $1000, I suppose, since we can’t screen for killers like pancreatic and stomach cancers via conventional means.
However, even the Mayo Clinic’s best effort does not stand up all that well to scrutiny. Oncologist Dr. Vinay Prasad co-authored a scathing piece on Galleri, primarily noting that even at a low 0.5% false positive rate, on a population level, screening everyone would lead to far more expensive, anxiety-provoking, and test-triggering cancer diagnoses than “saves” via early treatment. Without a prospective trial to see if screening people for every possible cancer really prevents cancer morbidity and mortality, it’s little more than an educated guess that trying to catch cancers early is really a winner, on a population level.
I would go even further, on an individual level. We really don’t know what to do with a negative Galleri test. The worst cancers are aggressive, and grow and metastasize rapidly. Would an annual screen catch most pancreatic cancers while they could still be resected locally? Probably not, I suspect. We don’t know, of course, because no one wants to spend the money and burn the time on a multi-year, randomized controlled trial on these tests. So maybe for those deadly cancers for which we lack other screening programs, we’d need to test every 6 months, or even 3?
False positive tests would then come into play. Not only is that a lot of money, but suddenly the reassurance of that 1/200 false positive rate starts to waver. If I begin screening my patients at age 40, twice annually until they die in their sleep at 90, that’s 100 Galleri tests in their lifetime. A false positive becomes a real risk — and what a nightmare! Can you imagine being told you probably have cancer, because the test is almost always accurate when positive, and then the colonoscopy, the PSA or mammogram, the skin survey and biopsies of every mole, the endoscopy, the CT chest, the CT abdomen/pelvis — all come back negative, and deep down you just know you have a tumor in there somewhere, resisting all efforts to find it?
No, thank you.
I might recommend a test like Galleri to a patient with a very high risk of cancers for which we cannot screen, based on family history or genetic screening. I would not recommend it for the general public, barring far better data than we now have.
There does seem to be a confluence of research and product development in this field in the past few years. That Stem Cells paper which seemed to draw the attention of the New York Post made sure to list ten competitors in its Supplement (only after pointing out all their shortcomings in the body of the piece). I’m not certain that this technology will ever rightfully supplement or even supplant our current underwhelming cancer screening programs, but I am hopeful.
As to the HrC test, it is now available in India for 14,000 Rupees (about $170), and reportedly coming soon to the UK, courtesy of the recently-incorporated “Accendo Supplies LTD.” The financial appeal of backing a test like this is obvious; its co-founder and CEO, Ashish Tripathi, speaks of wanting to screen 8 billion people annually. Now, that’s a good business model! Unlike the Galleri and its admitted poor sensitivity, however, HrC’s audacious claim of never missing an existing cancer, and giving you a one year safety blanket before these stem cells could even start to form a tumor, could really inspire patients with a negative result to disregard standard cancer screening.
Barring scientists without financial ties to Tzar Labs replicating their astoundingly positive results, I would not recommend this test to anyone. The HrC could turn out to be independently verified as a decent test; the company says further studies are underway. However, I am virtually certain that the results they currently trumpet are too good to be true.
I would rather be wrong than right about this. However, staking out the position that “nothing in medicine is perfect” is about the most reliable opinion a physician can offer.
April 22, 2023 Update: I have indeed been in email communication with one of the paper authors, Dr. Deepa Bhartiya, and am convinced of her sincere belief in the revolutionary potential of VSELs in detecting cancer. However, I have become even more convinced that the wool is being pulled over our eyes! This blog post from someone (unlike me) with actual in-field expertise raises questions over the very existence of VSELs, and mentions these very concerning allegations that one of the founding scientists behind VSEL research has engaged in fraudulent conduct (although his research institution has defended his research). If the existence and role of VSELs in cancer formation were fully recognized by mainstream scientists, I would still treat the results of the HrC testing with near-complete suspicion, given their perfection in an impossible field. Seeing these further doubts, I move from “near-complete” to “complete.”
Deja vu to PSA, anyone? Just because a test is there does not mean it should be used for widespread screening. And this particular test should not be allowed for general use based on a single study funded by the same people looking to make serious money if the test turns out to be marketable. Hopefully the regulators actually do their job and disallow this test to market without multiple other independent studies (preferably from other countries, totally unaffiliated, with no profit motive) confirming its results.
Repeating studies is not sexy and is not career making. But, isn't this why we have public funding for such research?
Due to the fact that I was diagnosed with dermatomyositis my rheumatologist insisted on follow up studies. After endoscopy, colonoscopy, two MRIs, visits with pulmonology, dermatology and oncology I was told things were fine. However, a much more informed dermatologist at our local medical center, with a veritable encyclopedic knowledge of dermatomyositis, insisted I see an oncologist on the medical center staff. This, rather young, oncologist reviewed all the findings and agreed they revealed nothing to worry about. However, he strongly recommended that I have a Galleri panel performed, which, of course, insurance wouldn’t cover. I followed his advice and the test came back positive for a head and neck cancer. Subsequently, ENT found an HPV associated SCCa on the base of the tongue. (Somewhat ironic since my specialty is oral pathology). After a course of chemo and radiation, PET scan shows no evidence of tumor.
So, while my scientific background compels me to agree with your surmise concerning the accuracy of the test I, for one, am eternally grateful that this young oncologist pushed me to have it done. Skepticism is the chastity belt of the intellect (and thusly science) George Santayana said, but one must be cautious not to allow for rigidity to acceptance of novel ideas. Let’s allow the science to play out. I strongly suspect the Galleri test will become routine in the future.