Does Urolithin A Work as a Muscle-Building Supplement?
The hype is outlifting the data.


I was listening to a podcast between two MDs the other day, curious to hear what they considered their “top supplements.” They listed the usual suspects — fish oil, magnesium, vitamins D3 and K2 — but top of the list was… urolithin A.
Huh?
I consider myself a supplement-savvy physician, but I had to find the rewind button. “Uro-what???” I had never even heard of urolithin A, and here it was: The. Most. Exciting. Supplement. Out. There.
After getting over my feelings of inadequacy and ignorance, I was curious enough to look up what we know about urolithin A. What I found was a cautionary tale of how a supplement maker can influence research and commentary in support of their product, not all that differently from what we are used to seeing from the pharmaceutical industry.
First, full disclosure: I don’t have any grudges against the Swiss firm, Amazentis, which makes the Mitopure Urolotihin A supplement, nor its investors and supporters, which include Nestle, Novartis, and even Elon Musk’s mom. I also am generally supportive of using supplements relative to many of my medical colleagues, especially in situations in which the pharmaceutical industry has failed to deliver good options (i.e., osteoarthritis) or when my patients are simply pharma-phobic, and strongly prefer “natural” options. I find a fair number of supplements are out there with decent trial evidence and a good track record with my patients, among them red yeast rice for high cholesterol, berberine for elevated blood sugars, and rauwolfia for hypertension. The nice thing about these examples is that they are easy to track — either the number in question improves or it doesn’t.
Urolithin A falls in a different category. It’s hard to find an objective measure for whether someone is feeling more youthful, less “pro-inflammatory,” or stronger. That’s the pitch, though.
Urolithin A is a metabolite of foods like pomegranate, broken down by our own gut bacteria in people blessed with a healthy gut biome, with the reputed property of pruning our mitochondria, the energy suppliers to our cells. The claim — and we see this, rightly or wrongly, for many supplements — is that most of us just don’t produce enough urolothin A to benefit from dietary sources alone. Hence, the biological mechanism: urolithin A will optimize our mitochondria and help us aging humans improve our strength and vitality!
The question, of course, is whether this actually happens. To that effect, I could find a series of studies dating back to this one in 2016, establishing that urolithin A’s effect on mitochondria improved longevity in worms and muscle function in mice; another the next year, finding supplementation with urolithin A was safe in rats; one in 2019 showing safety in humans, as well as improved mitochondrial biomarkers; a review article in 2021 on the benefits of urolithin A for protecting against age-related conditions; and the real breakthrough in January 2022, a randomized clinical trial based at the University of Washington and published in the JAMA Open Network, concluding “…long-term urolithin A supplementation was beneficial for muscle endurance and plasma biomarkers, suggesting that urolithin A may counteract age-associated muscle decline.”
This one kicked up some hype; for example:

You can see why a busy physician with a soft spot for supplements might start recommending urolithin A for their older patients. Multiple studies published in peer-reviewed journals; that’s a lot of reliable evidence, right?
Unfortunately, there’s a catch. Really, a few.
First of all, all those laboratory and clinical studies I listed? The names of the same researchers keep popping up in every one; most of all, Dr. Chris Rinsch, the, um, CEO and co-founder of Amazentis. In fact, the Amazentis “team” —
— bears a striking resemblance to the authorship of the JAMA article (and the others before it):

Much as I don’t like it when the only trials on Paxlovid are run by Pfizer, when all the work on a supplement is run and financed by the only company producing said supplement, I get nervous. It’s not that either Pfizer or Amazentis is presumed to be cheating to get positive data; but they can be presumed to be designing studies with the highest likelihood of producing positive results, and reporting on them with maximum favorable spin.
With that in mind, Amazentis can now claim forever that their Mitopure Urolithin A product (3 month starter pack: $300) has “clinically proven” results, published in one of the most respected journals in medicine. In a parallel universe in which I did not have a free morning to pick apart the history of urolithin A, if a patient asked me if they should try it, and I only had a few minutes to look it up and glanced at the abstract from JAMA, I ‘d probably say, “sure, it’s worth a shot.”
However, I now live in the universe in which I read through that article, and that’s not the advice I would give.
Without digging too deeply into the details of a 12-page study (which can be found here), I’ll say that a few concerns jump out. One is that there were multiple markers studied (muscle endurance, 6 minute walk distance, muscle ATP production, two mitochondrial health biomarkers, and an inflammatory marker), sometimes at two body areas (hand and leg), often at 2 time points (2 and 4 months). This leads to A LOT of potential end points upon which to claim success if what you really have is a product that relies more on random chance than actual biological effect. This is exactly the sort of trial I would design if I were the CEO of the company making the supplement I was studying!
Another concern is that the primary endpoints were changed after the trial design had been established. This falls in the “no-no” category.

No major shaming here, though, as the real issue with the study is that, despite shifting the goalposts mid-game, it failed. Positive conclusions and spin aside, it failed to show any real benefit.
6 minute walk distance did improve by 15%; but placebo improved 10%, a non-significant difference. ATP production showed no difference at all between placebo and urolithin A. Muscle endurance was improved in the urolithin A group at 2 months, but placebo caught up by month 4 to erase any statistical significance. Yes, the 11 acetylcarnitines and 2 ceramides tested showed modest 5-20% reductions on average, but I am confident that no one in the Universe knows if that has any clinical relevance whatsoever to actual mitochondrial health.
Perhaps most strangely, the authors trumpet an improvement in inflammatory markers based on a reduction of C-Reaction Protein (“CRP”) in the urolithin group from 2.14 to 2.07.

For those unfamiliar with CRP, it is one of the most variable laboratory tests in common use; it’s not unusual to see a patient shift from a healthy 0.5 to a suboptimal 2.5 in the space of 6 months, and if that patient gets a bad cold or skin infection, it could race up to 10 or 50. There is simply no way a tiny reduction (0.07mg/L) among a mere 33 participants could be a statistically significant result. Granted, based on the image included in the Supplement, I believe this to be a typo, and the actual reduction is more likely from 2.65 to 2.07; but still, I strongly doubt this modest change in a highly variable biomarker amounts to a clinically significant result.
{kind=link}
So, there we have it. Swiss firm finds a possibly useful natural compound, devotes years of laboratory and then clinical research to it, raises millions of dollars from investors, and finally has a breakthrough randomized controlled trial on it, which shows… practically nothing. Their reward? Somehow JAMA Network Open’s peer review process allows them to run this as the “Key Points” at the top of the page:
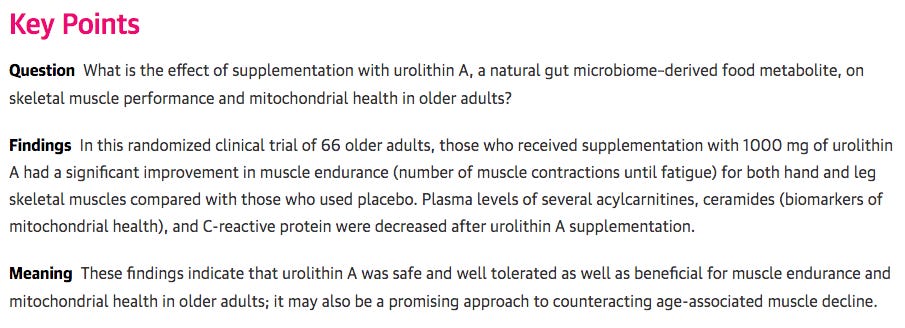
This, despite the claims being largely refuted by their own “Results” section farther down. It’s odd, and JAMA should do better. In fact, I’m rather surprised a trial of this quality was published at all. Maybe Elon Musk’s mom knows someone.
Of course, it’s possible Dr. Rinsch and his team are onto something, and their supplement just had an off trial. Much more likely, though, is that urolithin A has somewhere between “no benefit” and “virtually no benefit” when ingested by aging humans hoping to feel stronger and more vital.
I can think of better ways for my patients to spend a spare $100/month to improve their strength and vitality. A gym membership, or produce share boxes from a local farm, come to mind. However, I am aware that the Medical-industrial complex would not support this message.
The problem with the same authors repeatedly publishing articles extends far beyond medicine. I looked at every article ever published about Dunning-Kruger Syndrome (sociology) and either Dunning or Kruger was credited as an author on 90%.
The only study to duplicate the original results used dummy data.