
President Biden's Paxlovid & the Problem with Overtreatment
"It might just help" is not a good enough reason to prescribe a medication.

You may have heard: President Biden got Covid. You may also have heard: he took Paxlovid, got better, tested negative a few days, and then started testing positive again with a bit of a cough. Did the twice-vaccinated, twice-boosted Biden need Paxlovid to treat his mild Covid symptoms to avoid severe disease? Probably not. Could we have predicted the risk that Paxlovid might lengthen his disease course, make others vulnerable to contracting Covid during a possible rebound, and put the President at a slightly higher risk of stroke due to the need to hold his anticoagulants for a week? Definitely.
So why did his doctors put him on it despite the obvious concerns? After all, this man should have the best medical care in the world. The problem, especially for important patients who want to get well as fast as possible, lies in the pressure for physicians to overtreat our patients. Doing nothing, even when the best course, is rarely a popular option.
Now, despite the fact that the most intimate details of our president’s health are freely available for all to review, we doctors are discouraged from getting involved in the diagnosis or treatment of public figures. I would never do this. However, we might find a lesson or two in the story of how a hypothetical 79-year-old man, fully vaccinated, on two important heart medications for his atrial fibrillation and high cholesterol (Eliquis and Crestor) that would need to be held for a possible course of Paxlovid, still ends up being given the controversial antiviral.
Of course, recommending Paxlovid to our 79-year-old patient is well within its Emergency Use Authorization. Anyone over 12 years of age at “high risk for progression to severe Covid-19” is deemed appropriate. Of course, we physicians (and now pharmacists) are left to determine who exactly is at high risk.
Back in the long-ago days when the original Wuhan strain was circulating, and few people had immunity, we had risk calculators that were probably fairly accurate. A 79-year-old man with a heart condition would have been thought to have a risk of a severe case of Covid-19 north of 30%. Now, with a less virulent variant that tends to stay out of people’s lungs, and widespread immunity via vaccinations and infections, no one has a hard number for estimated risk of hospitalization or death.
That does not stop my patients from asking, though, often in the context of inquiring about a Paxlovid prescription. I look at state data for official cases by age group (about 200 reported cases per 100,000 seniors over 65 per week at the BA.5 peak), multiply by seven per the IHME to allow for unreported infections (though I suspect that multiplier is far too low), and divide into COVID-NET’s national rates for hospitalizations in the 75-84 age group (about 40 per 100,000 per week), cut in half in an attempt to avoid counting incidental admissions. The very crude ballpark infection hospitalization rate that results for this cohort of average health, mostly vaccinated Americans around 80 years old, comes out a little under 1.5%.
This roughly fits the old Economist risk calculator, in that a 30% risk of hospitalization per case should be dropped to about 3-5% via full vaccination and two boosters, and Omicron should drop the risk further by a factor of 2-3. It also passes the eye test; given the incredible prevalence of BA.5 everyone certainly noticed in the past couple months, our hospitals would be full to the brim if the elderly were being admitted for Covid infections at anything like a 30%, or 10%, or even 5% clip.
Now, is a man who ostensibly receives the best medical care in the world, capable of performing the most challenging job in the country (I am not going to editorialize on a certain someone’s job performance here), with a fairly common heart problem in otherwise fine health, really anywhere near “average” risk? I would imagine his doctors would estimate his risk of severe disease from Covid-19 to be under 1%.
So — where does Paxlovid fit in, in terms of reducing risk in a “high risk” person who is flush with four vaccines? The honest answer is: we have no idea.
The stunning success of Paxlovid’s EPIC-HR (as in, “High Risk”) randomized controlled trial took place during the reign of Delta, and included only high risk patients who were unvaccinated. Severe disease and death were reduced by nearly 90% in the Paxlovid group vs placebo. A remarkable achievement in the realm of antivirals, but, as Dr John Mandrola asks in this piece, perhaps it does not translate out into the real world we now inhabit, in which almost everyone has immunity, and the variant du jour is BA.5.
It certainly is plausible that most of Paxlovid’s value as an inhibitor of viral replication would be seen in people poorly equipped to mount an early immune response. Immune competent hosts with immunity from, say, 4 vaccines, or a prior infection or two, probably respond rapidly to an Omicron infection; the well-known phenomenon of vaccinated people having symptoms 2-3 days before seeing enough viral load to even test positive on a rapid test might imply this to be the case. Possibly, the immune response is so rapid and effective that there is little advantage to be gained by adding a medication that inhibits viral replication.
Unfortunately, we have scant evidence upon which to form an opinion for this cohort. A large study from Hong Kong showed a reduction in hospitalization among Paxlovid users vs non-users of 31% — and 39% among vaccinated people — but most of the elderly there are vaccinated with the less effective Sinovac vaccine. Then we have a more promising study from Israel, in which patients over 60 given Paxlovid experienced a 48% reduction in severe disease compared to those not given Paxlovid. (Those under 60 saw no benefit at all, yet another reason not to try to cadge a Paxlovid prescription if you are reasonably young and in decent health). For vaccinated people, the benefit was a more modest 38%. Results below:
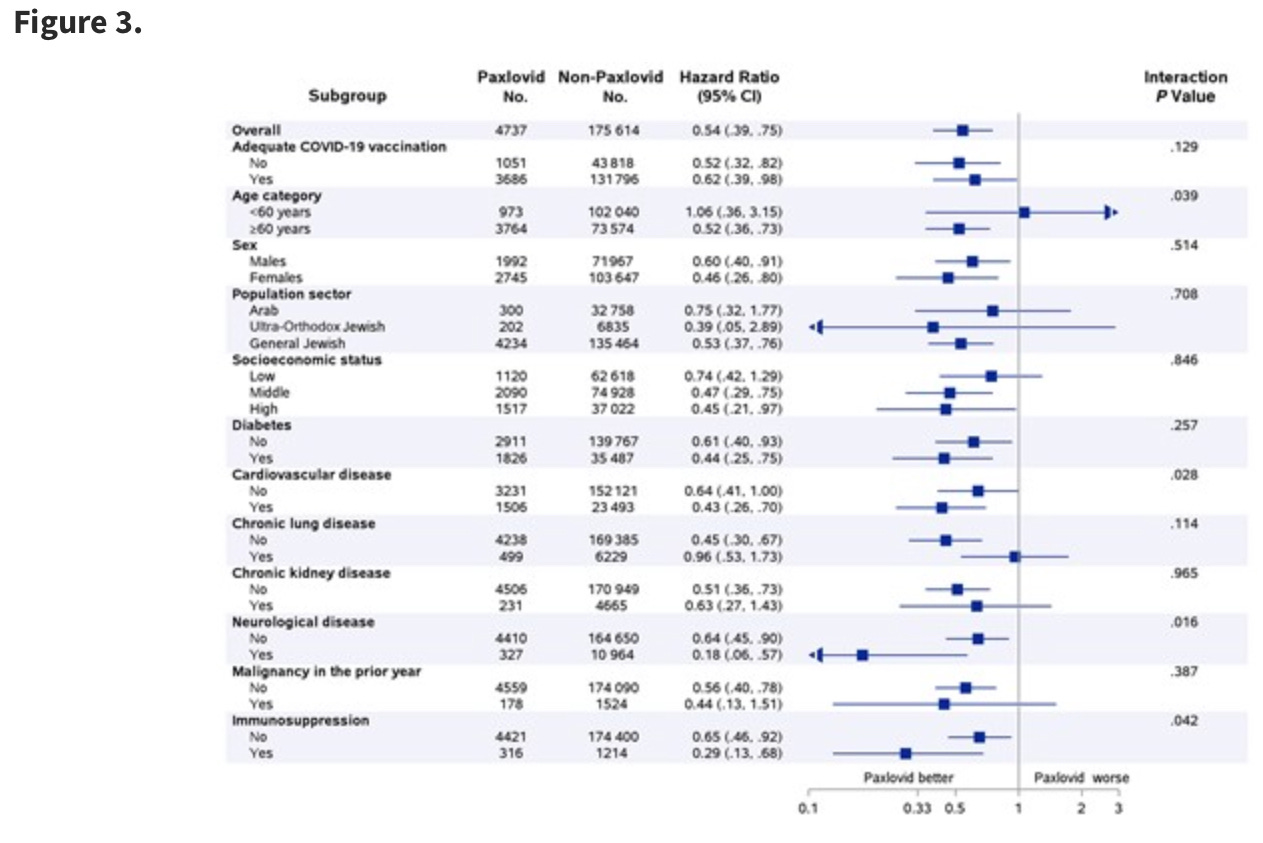
Of course, this was no randomized controlled trial, but rather a retrospective observational trial, meaning some people got Paxlovid, and others didn’t, and the authors compared how they fared. The Paxlovid group actually ended up hospitalized at twice the clip of those that did not, but as they were older (68 vs 54 years old, on average) and a third as likely to be Arab, the authors adjusted these raw numbers to reach the results stated above. The concern, as with any observational trial, is that certain variances cannot be adjusted away. Perhaps the sort of Arab in Israel with access to Paxlovid is just less likely to have a bad health outcome; or a member of the general Jewish population with diabetes who gets Paxlovid has better access to care in general than a diabetic Jew who does not get that prescription.
Another preprint from Massachusetts shared similar results from a similarly large study; a 45% reduction in hospitalization for those who received Paxlovid vs those who did not, falling to a 28% reduction among vaccinated patients. Again, those who got Paxlovid tended to be older, whiter, and have more comorbidities; are there hidden confounders behind who has access to a coveted Paxlovid prescription? We can’t know, and no amount of regression modeling can save us. This is why we need randomized controlled trials!
Well, we almost got one. The EPIC-SR (“Standard Risk”) trial was intended to answer the question of how moderate risk unvaccinated people and higher risk vaccinated people would benefit from Paxlovid. Still pre-Omicron, but a much more useful gauge of where a quadruple-vaccinated 79 year old needs Paxlovid. The result? We don’t know. The trial was stopped partway due to clinically insignificant results and low rates of the important outcome, hospitalizations, in both groups. Headlines were uninspiring:

One thing we can probably assume is that the trial was not going well for Pfizer, and prospects for improvement were dim. Indeed, the primary endpoint, symptomatic improvement sustained for 4 days, was no better for those taking Paxlovid than placebo.
That’s worth a thought. The current conventional wisdom seems to be, “people forget that Paxlovid is for preventing severe disease.” Apparently Pfizer did not think so when they designed this trial; and I think most of my patients want Paxlovid so they can, y’know, feel better sooner. People don’t clamor for Tamiflu because they think they are going to die of the flu; they just don’t do want to be really sick. I also worry that Paxlovid not reducing illness duration in this more immune-robust cohort is a sign that it doesn’t really prevent severe disease, either.
The results from the aborted trial offer a glimmer of hope in this regard; there was a 57% reduction in severe disease among the vaccinated with risk factors for disease progression, but it was not statistically significant, and was trending downward from their initial read-out the earlier in the study. Keeping in mind that this was Pfizer’s study, and they did not even want to finish it, I really think it important to take that 57% reduction with a large grain of salt, as probably a very high end figure for this purpose.
With this as a backdrop, I cringe when I hear people defend President Biden taking Paxlovid by regurgitating that Paxlovid reduces hospitalizations by 90%.

What does that 90% have to do with the present tense? The Pittsburgh Steelers were pre-season favorites to win the Super Bowl in 1978, but I will not leverage this information to lay a wager on their 2022 incarnation.
In the Israel study of 180,000 high-risk Covid patients (only about 5000 patients actually received Paxlovid), the rate of hospitalization was only 0.5%. That figure was under 1% in the Massachusetts study. In the pre-Omicron Pfizer EPIC-SR study that included high-risk vaccinated patients, 1.8% of placebo patients experienced a severe outcome. I observe that these figures, while obtained from studies with median ages in the 50s and 60s, are based entirely on formally diagnosed cases. Were Joe Biden a Joe Smith, would his cold symptoms have led to a laboratory diagnosed, reported case of Covid? Probably not.
I suspect the ballpark of 1% hospitalization risk for a 79-year-old man in good overall health is probably not far from the mark. It’s important to note that, even if our best case scenario is true — that the Israel, Massachusetts and EPIC-SR data can be extrapolated to estimate, say, a 40% reduction in risk — the absolute risk reduction, from around 1% dropped to 0.6%, is tiny. Among 250 parallel universe “to treat or not to treat” scenarios, the Paxlovid course would save a single hospitalization. The question, always, is whether that small gain is worth it.
On a societal level, it gets expensive to push out 250 definite $600 treatments to save one possible hospitalization. On a personal level, the concern is harm.
Paxlovid side effects, like changes in taste, are mostly annoyances. I have already spoken my piece about Paxlovid rebound; it’s probably common, presents problems with prolonged periods of contagion, and raises questions about whether hitting a temporary pause on viral replication might hamper our immune response towards future infections, or possibly increase our likelihood of developing long COVID. These concerns worry me. Still, they are hardly a deal-breaker when there is real concern for high risk of severe disease. However, the need to stop the multitude of medications which interact with Paxlovid can create real dilemmas.
In the case of someone taking a blood thinner like Eliquis to prevent stroke, stopping an anticoagulant for a week carries some small but undeniable increased risk of a stroke. We know viral illnesses can precipitate a stroke, and SARS-CoV-2 especially so. While the risk of stroke in that window of time with reduced anticoagulation would be extremely low, certainly under 1% and perhaps a fraction even of that (based on annual stroke incidence in the 3-10% range for most elderly people with atrial fibrillation), I don’t need to say that a stroke afflicting this particular 79-year-old man would be devastating, much more so than a 4-day hospitalization for viral pneumonia.
In short, this would be a dilemma. If you buy that even a twice-boosted immunocompetent person has a 40% ballpark risk reduction in severe disease from a course of Paxlovid, and you assess their risk of severe disease to be more like 5% than 1%, you would rationally choose to prescribe the Paxlovid. I, however, think the risk reduction in this case is closer to zero than 40%, and the baseline risk from Covid so low, that the cost of holding both a statin and an anticoagulant would exceed benefit, and the downside risk more catastrophic than the hospitalization that was hoped to be averted.
Of course, there is never a right answer revealed in scenarios such as this. The end result - a president with a case of Paxlovid rebound, who likely would have been over his infection and the concomitant risks by now had his doctors shown more prescribing restraint - does not provide a winner to the debate. I can say that my personal philosophy with Paxlovid among my vaccinated or previously-infected patients is to discourage its use unless they are extremely frail or immunocompromised; or if their clinical course appears to trend towards that rare case of Omicron that deteriorates towards hospitalization. Perhaps the presidential physicians could have waited for a sign of clinical worsening before starting a prescription.
In any case, it’s a healthy reminder that sometimes the best course in medicine is to prescribe nothing. An outstanding example is the use of antibiotics for sinus infection. They provide almost no advantage over tincture of time, but can lead to a host of adverse reactions, from antibiotic resistance to gut biome disruption to sunburns to increased risk of diabetes. The risks almost always outweigh the benefits. And yet, it is almost impossible to walk into an urgent care clinic complaining of sinus pain without walking out with an antibiotic prescription.
Over-treatment will never go away, and will penetrate into the highest offices of medical practice. Patients are wise to ask their doctors: “What are the outcomes if I don’t take the medicine compared to if I do?” I preach to my patients to badger their specialists until they get an answer; every single doctor making every single medical decision has a ballpark risk:benefit number in their mind before rendering their advice. We all have those numbers tucked in a cerebral fold somewhere, even if we don’t like having to justify our rationale.
In the case of President Biden and his Paxlovid prescription, I think their numbers were off.
I pity any doctor who faces so many treatment options for the seemingly never ending march of Covid variations, Dr. Hollander.
My wife is a CRNA with about 35 years of experience. During the worst of the pandemic she was always on the wrong side of the sterile barrier. Double N95 masks plus plastic welder style shields were the order of the day for anesthesia providers, and yes, she did having a pregnant woman fib about not having eaten. The result was vomit hitting my wife's mouth, nose and eyes.
I should mention that my wife is 15 years younger than my soon approaching 79 years, and thus much more healthy than me.
Being married to a medical professional at Advent Health in Ocala, FL made it possible for me to get my Moderna shots just after Christmas of 2020 and the end of January of 2021. In December of 2021 I received a Moderna booster.
After attending a national volleyball tournament in Orlando in June that included our granddaughter's team, I caught Covid for the first time.
Once again, Nurse Mary came to the rescue, opening a Covid test kit as soon as we got home.
She forced me to drink what seemed like a gallon of water and half a gallon of OJ.
She then called our family doctor to get access to the drug regime used at her hospital for patients who are within the first 24-36 hours of exposure.
Because of my age and my half century smoking habit she got a prescription for an 10 day course of antibiotics to keep my lungs functioning, 20 milligram of prednisone, and several other meds I cannot remember.
My fever and other symptoms cleared out within three days.
I'm sharing this information to illustrate how how many variables go into treating the Covid variations. I suspect I would not have fared so well had I not been married to a spouse with broad experience dealing with the pandemic.
When President Biden came down with Covid, my wife's initial reaction about Paxlovid was similar to yours.
I appreciate your articles dealing with Covid and other complex medical issues for those of us who barely crept up to a B- when we took Biology 101 and Chemistry 101 so long ago.
Thank you for "Buzzing" us periodically.
After two years of almost daily cringing at the arrogance, dishonesty, and incompetence of Fauci, Levine, Walensky and Birx, the notion that Biden is getting great medical care is laughable. These people have set the cause of trusted physicians back a generation.