

The New Polio Outbreak Is Bad. But Why Hasn't It Become a Disaster (Yet)?
Despite what you might read, polio’s return in unvaccinated pockets outside NYC is anything but predictable or obvious.

Viruses are fascinating. Watching the twists and turns of SARS-CoV-2 mutations and their effect on the entire planet has made it easy to appreciate the raw evolutionary ability of a novel viral pathogen. But polio… there’s a virus with some serious history on its side, from Egyptian carvings to FDR’s wheelchair, and it’s still grabbing headlines.
The latest:
It’s easy to feel a bit of panic in the air. A young man was paralyzed in the New York City suburbs. Poliovirus was found in the wastewater of 8 boroughs of London. What in Sam Hill is going on here?
To understand, I had to do some reading. Whatever little bit I learned about polio in med school I promptly forgot, since, well, no one sees polio anymore. Vaccines made the worst-case, 1 in 200, outcome of a poliovirus infection, paralytic poliomyelitis, virtually disappear. Not totally, however, and that’s where this virus and the vaccines that prevent it get so interesting. So much so that it’s worth breaking it down a little, to get a better handle on why it popped up in a New York City suburb, and what that means to us going forward.
Interesting Polio Vaccine Fact #1: The Salk vaccine, generally known as the inactivated polio vaccine (IPV), developed first and used exclusively in the US since 2000, is incredibly effective (99%+) at preventing paralytic poliomyelitis but does not convey mucosal immunity, and therefore does little to reduce transmission of the poliovirus.
Yes, a true life-saving, disability-sparing vaccine, and one with virtually no adverse effects. However, the inactivated virus triggers a marvelous immune response in the blood without establishing immunity in the gut. Since poliovirus is a fecal-oral route pathogen — meaning viral particles are not passed in tiny aerosols from our breath, or large droplets from a cough, but rather in tiny bits of fecal matter that make their way onto hands, or into the water supply, and then into mouths — the poliovirus can readily spread itself in its usual manner among a population entirely immunized via the IPV vaccine. Remember that, Americans! Lest we think our adult selves too clean for such a lowly route of transmission, recall that we are a “wipe right/shake right” society, and that not every food preparer employs ideal hand washing technique in the restaurant bathroom.
When you see Science reporting like this, you might want to unsubscribe; this quite misconstrues the protection actually afforded to a country well-vaccinated via IPV:

The New York Times offered a similarly poor characterization; it’s fair to fault communities with low IPV uptake for putting their populace at risk, but not for spreading the disease:
Interesting Polio Vaccine Fact #2: The live attenuated Oral Polio Vaccine, developed by Dr. Albert Sabin, is cheap, easy (taken as a few drops of liquid by mouth), and remarkably effective both at preventing infection in the gut as well as severe neurological disease, but has an Achilles heel: it can mutate back into a virulent form of polio!
This is the vaccine that has virtually eliminated wild-type polio from the globe. In the US, it was used exclusively for decades until polio was essentially gone, and then IPV reintroduced. Why bring back the older, more expensive IPV? The faint risk of vaccine-associated paralytic polio (VAPP). Very rarely — in the 1 in 2-3 million range — people who receive the vaccine, often immune-compromised, brew up a case of paralyzing poliomyelitis if the virus mutates into a pathogenic form and attacks the nervous system. Sometimes, too, especially in communities employing the OPV vaccine but with lower rates of acceptance, a strain could circulate among the community and acquire mutations over a year or two that would revert it back to a pathogenic strain, so-called “circulating vaccine-derived poliovirus” (cVDPV). The treatment, at least until 2020, was to give everybody more OPV until herd immunity is built up and hope to avoid more vaccine-associated or vaccine-derived cases of polio!
Interesting Polio Vaccine Fact #3: There are 3 types of wild poliovirus; type 2 has been eradicated (and recently type 3 as well) through the global OPV campaign, but type 2 most easily mutates back into a virulent form from the OPV vaccine, meaning that no wild type 2 poliovirus is now in existence, but most cases of actual poliomyelitis are caused by vaccine-derived type 2 polioviruses.
This has led to a wild cat-and-mouse game between vaccine-derived virus and vaccine. Bivalent (type 1 and 3 only) OPV was developed, since wild type 2 was eliminated from the globe and the type 2 strain in the vaccine was so problematic. Great — except when a vaccine-derived type 2 strain begins to circulate in an undervaccinated community! Neither existing option was appealing: either bring in IPV (not always possible in the developing world) only to prevent paralytic disease without breaking transmission chains, or saturate the community with the old trivalent OPV vaccine and risk more of the same problem in the future. The solution to this cycle has been the development of a modified type 2 monovalent OPV (mOPV2), reformulated to greatly reduce the risk of mutating into a problematic form. This is the new band-aid for outbreaks of vaccine-derived poliovirus since 2020; but of course will not protect against the type 1 wild poliovirus still found in Afghanistan and Pakistan, nor the type 3 vaccine-derived poliovirus found circulating in Israel that led to paralysis in a 3 year-old earlier this year.
Speaking of Israel, it appears to be a poorly-kept secret (since the New York Times reported it) that the young man now paralyzed with poliomyelitis from a type 2 vaccine-derived poliovirus is a member of the Orthodox Jewish community. Yes, that Orthodox Jewish community in Rockland and Orange Counties, with the notoriously low rate of childhood vaccinations (around 60%) that went through a measles outbreak in 2018-19.
If we were in Africa or India, the sensible public health response would have been to bring mOPV2 into the community health centers, and have the rabbis begging their synagogues to have everyone immunized with this ideal vaccine to both stop the spread of this strain and prevent severe disease. Instead, in a move that appears to leave virologists somewhere on the spectrum between bemused and bedeviled, we stick with IPV, allowing transmission to continue almost unabated. But at least we publicize it!

The problem, of course, is that while paralysis will be prevented in people, like the gentleman pictured above, who get their IPV vaccine, there can be no herd immunity via these vaccines for those who can’t be persuaded to roll up their sleeves, given the lack of mucosal immunity. From what I can tell, this creates a problem; observe the reproductive number of polio in a non-immune community:
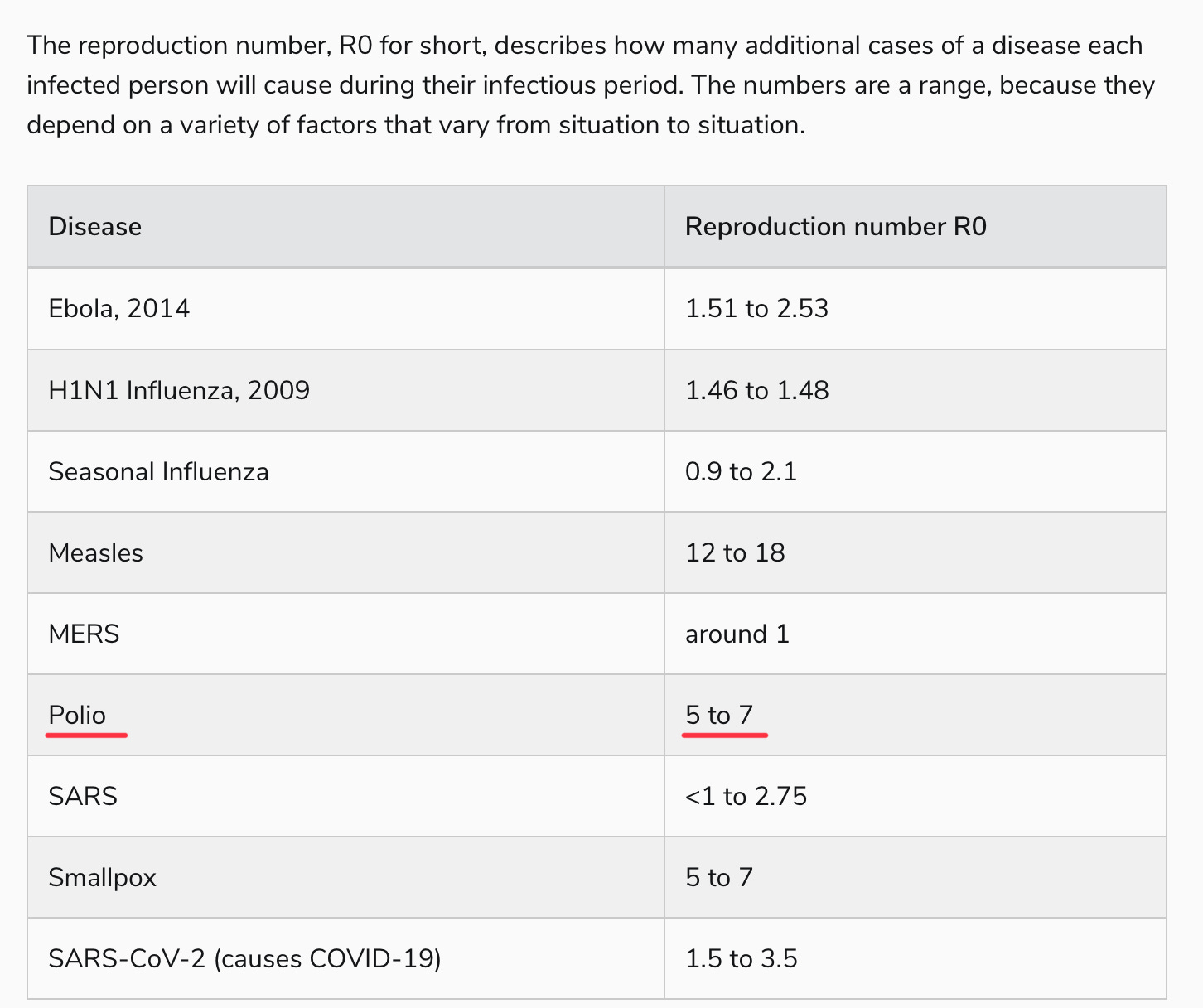
Yes, polio is right up there with our most transmissible pathogens, probably not far from our new friend, Omicron BA.5. Perhaps this is outdated information, calculated in an era of open sewers, or simply overstated. But hearing virologists talk about polio, it’s generally with a sense of, “oh, everyone just gets it” in outbreak conditions, which is why a paralytic polio rate of 1 in 200, or even 1 in 1000, is so problematic.
That, to me, is the mystery of these recent vaccine-derived polio outbreaks. The protection against polio infection — not paralytic poliomyelitis, mind you, just the majority of poliovirus infections which are asymptomatic (around 70-75%) or the remainder that are more flu-like — should be incredibly low, at least among those born after 2000 in the U.S. who are not blessed with the superior immunity of OPV recipients. How does a virus with an R0 >5 circulate for months in places like New York and London without tearing through the kids in a densely-packed, non-immune community, and not rapidly spread to other communities?
It strikes me that we have either been exceedingly lucky to have not heard of more than 2 cases of paralytic polio since reports began to circulate 6 months ago; or the circulating vaccine-derived strains are either less transmissible or less virulent than we imagine them to be. I freely admit that I am just spitballing here; when I look through the literature there seems to be consensus to the contrary, that the mutations in past vaccine-derived poliovirus made it just as formidably transmissible and virulent as the wild-type polioviruses.
Perhaps the New York outbreak will yet lead to a massive polio outbreak, unlike the warnings thus far raised in London and Jerusalem. Meanwhile, I await a virologist to explain the seeming contradiction between the disaster we would expect from these emergent strains in multiple countries and what we are actually seeing. Truly, like so much in medical science, it’s a mystery.
What is not at all mysterious is the appropriate response to these reports of circulating polioviruses. Yes: vaccination! Here in the U.S., we can’t invoke vaccine mandates and herd immunity to stop a potentially massive outbreak of a vaccine-derived poliovirus, at least not without authorizing either new or old OPV vaccines for distribution. What we can do is make the problem go away in our own families via the IPV vaccine. It works, and it’s safe. To that effect, I can say that, as the current Giver of Vaccines in my clinic, I take full disclosure seriously, perhaps to a fault, because I don’t want parents to lose trust in medicine if they are blindsided by a vaccine reaction or read about terrible adverse events afterwards and feel misled by me. When it comes to IPV, though, I really struggle to come up with any concerns; maybe their arm might get sore?
With an effective vaccine with little risk, the inevitable question is finding its voice among older patients: “Should I get a polio booster?” This leads to one last interesting fact:
Interesting Polio Vaccine Fact #4: We really don’t know how long the immunity from polio vaccination lasts.
It’s true. Per the CDC, after IPV we’re “most likely protected for many years”:
After OPV, an Italian study estimated that we “should be protected for at least 18 years.”
Not exactly confidence-inspiring verbiage for those of us decades out from our last shot. I get it; it’s hard to find case reports of elderly patients contracting polio for the first time and becoming paralyzed. Is that due to adults being resistant to the worst effects of the poliovirus, though, or that the vast majority of adults in modern history were either fully vaccinated or exposed to poliovirus as children, and hardly exposed to poliovirus as adults? Another mystery.
I can say that we have case reports of paralytic poliomyelitis patients approaching my own advanced age of 52; and the example of FDR, controversial as it may be, diagnosed at 39. For an adult, especially one living around a polio outbreak, doubly so if they’re not sure they got a complete polio series as a child or have any doubts about their immune system, why not get a booster?
This is a scene I don’t even want in my nightmares:

Lets please admit that medicine really doesn't understand much about immunity, contagion and especially vaccination. The polio vaccine isn't sterilizing? It may only "work" for a few years? Doctors didn't know this, patients didn't know this, politicians and the rabid pro-vax propaganda machine never knew this ( or much else). Ethically, a vaccine which doesn't prevent transmission should never be mandated. People should get the polio vaccine if they think it will protesct against paralysis.
But how many vaccines is too many? What does all this messing with the immune system do? No one knows, and please dont tell me they do. I have spoken with a top scientist formerly on the FDA vaccine safety commission. You can guess who it might be. He said HepB should not be given at birth . He had plenty to say about covid vax too, none of it good.
Lets start with a little more humility from the public health authorities. And a little more respect for Nature. Primo non nocere!
vaccine-derived polio outbreaks are explained when you realise that the vax contains toxins and how toxins are the CAUSE. read this and think about where polio was found this time, in regions that have high jab rates, with unknown ingredients that produce a well known toxin (spike protein) this was written a few years a go and i cant find the author to thank them for making more sense than the virus theory:
let's take a look at history and polio!
1824: Metal workers had suffered for centuries from a paralysis similar to polio caused by the lead and arsenic in the metals they were working with. English scientist John Cooke observed: 'The fumes from these metals, or the receptance of them in solution into the stomach, often causes paralysis.'
1890: Lead arsenate pesticide started to be sprayed in the US up to 12 times every summer to kill codling moth on apple crops.
1892: Polio outbreaks began to occur in Vermont, an apple growing region. In his report the Government Inspector Dr. Charles Caverly noted that parents reported that some children fell ill after eating fruit. He stated that 'infantile paralysis usually occurred in families with more than one child, and as no efforts were made at isolation it was very certain it was non-contagious' (with only one child in the family having been struck).
1907: Calcium arsenate comes into use primarily on cotton crops.
1908: In a Massachusetts town with three cotton mills and apple orchards, 69 children suddenly fell ill with infantile paralysis.
1909: The UK bans apple imports from the States because of heavy lead arsenate residues.
1921: Franklin D. Roosevelt develops polio after swimming in Bay of Fundy, New Brunswick. Toxicity of water may have been due to pollution run-off.
1943: DDT is introduced, a neurotoxic pesticide. Over the next several years it comes into widespread use in American households. For example, wall paper impregnated with DDT was placed in children's bedrooms.
1943: A polio epidemic in the UK town of Broadstairs, Kent is linked to a local dairy where cows were washed down with DDT.
1944: Albert Sabin reports that a major cause of sickness and death of American troops based in the Philippines was poliomyelitis. US military camps there were sprayed daily with DDT to kill mosquitoes. Neighboring Philippine settlements were not affected.
1944: NIH reports that DDT damages the same anterior horn cells that are damaged in infantile paralysis.
1946: Gebhaedt shows polio seasonality correlates with fruit harvest.
1949: Endocrinologist Dr Morton Biskind, a practitioner and medical researcher, found that DDT causes 'lesions in the spinal cord similar to human polio.'
1950: US Public Health Industrial Hygiene Medical Director, J.G. Townsend, notes the similarity between parathion poisoning and polio and believes that some polio might be caused by eating fruits or vegetables with parathion residues.
1951: Dr. Biskind treats his polio patients as poisoning victims, removing toxins from food and environment, especially DDT contaminated milk and butter. Dr. Biskind writes: 'Although young animals are more susceptible to the effects of DDT than adults, so far as the available literature is concerned, it does not appear that the effects of such concentrations on infants and children have even been considered.'
1949-1951: Other doctors report they are having success treating polio with anti toxins used to treat poisoning, dimercaprol and ascorbic acid. Example: Dr. F. R. Klenner reported: 'In the poliomyelitis epidemic in North Carolina in 1948 60 cases of this disease came under our care... The treatment was massive doses of vitamin C every two to four hours. Children up to four years received vitamin C injection intramuscularly... All patients were clinically well after 72 hours.'
1950: Dr. Biskind presents evidence to the US Congress that pesticides were the major cause of polio epidemics. He is joined by Dr. Ralph Scobey who reported he found clear evidence of poisoning when analyzing chemical traces in the blood of polio victims.
Comment: This was a no no. The viral causation theory was not something to be questioned. The careers of prominent virologists and health authorities were threatened. Biskind and Scobey's ideas were subjected to ridicule.
1953: Clothes are moth-proofed by washing them in EQ-53, a formula containing DDT.
1953: Dr. Biskind writes: 'It was known by 1945 that DDT was stored in the body fat of mammals and appears in their milk... yet far from admitting a causal relationship between DDT and polio that is so obvious, which in any other field of biology would be instantly accepted, virtually the entire apparatus of communication, lay and scientific alike, has been devoted to denying, concealing, suppressing, distorting and attempts to convert into its opposite this overwhelming evidence. Libel, slander, and economic boycott have not been overlooked in this campaign.'
1954: Legislation recognizing the dangers of persistent pesticides is enacted, and a phase out of DDT in the US accelerates along with a shift of sales of DDT to third world countries.
(Note that DDT is phased out at the same time as widespread polio vaccinations begin. Saying that, polio cases sky rocket only in communities that accept the polio vaccine, as the polio vaccine is laced with heavy metals and other toxins, so the paralysis narrative starts all over again. As the polio vaccines cause huge spikes in polio, the misinformed public demand more polio vaccine and the cycle spirals skyward exponentially)
1956: the American Medical Association mandated that all licensed medical doctors could no longer classify polio as polio. All polio diagnosis would be rejected in favor of Guillian-Barre Syndrome, AFP (acute flaccid paralysis), Bell's Palsy, Cerebral Palsy, ALS, (Lou-Gehrig's Disease), MS, MD etc etc. This sleight of hand was fabricated with the sole intent of giving the public the impression that the polio vaccine was successful at decreasing polio or eradicating polio. The public bought this hook, line and sinker and to this very day, many pro vaccine arguments are ignited by the manufactured lie regarding the polio vaccine eradicating polio.
1962: Rachel Carson's Silent Spring is published.
1968: DDT registration cancelled for the US.
2008: Acute Flaccid Paralysis (AFP) is still a raging in many parts of the world where pesticide use is high, and DDT is still used. AFP. MS, MD, Bell's Palsy, cerebral palsy, ALS (Lou Gehrig's Disease), Guillian-Barre are all catch basket diagnosis, all similar in symtpoms, tied to heavy metal poisoning and high toxic load.
2008: WHO states on its website: 'There is no cure for polio. Its effects are irreversible.'
Conclusion: Modern belief that polio is caused by a virus is an ongoing tragedy for the children of the world. Public funds are wasted on useless and dangerous vaccines when the children could be treated with antitoxins. A call into failing vaccine mythology is warranted, as is a complete investigation of the real agenda being executed against humanity involving science, chemicals, vaccines, the medical field in general, and the government.