

Just Say NOvavax: Why Approve the Age 12-17 Novavax Vaccine That (Almost) No One Needs?
The FDA, acting without its advisory committee, rubber stamps a vaccine with real concerns for risk exceeding benefit.

I spent most of the last two weeks deep in the woods of the Pacific Northwest, deep enough to actually lack cellular reception. The world makes a lot more sense watching clouds roll past and marmots duck under rocks, at least more sense than FDA Covid-19 vaccine decisions. Unfortunately, a vacation has to end, and I have to transition from gazing at a scene like this on Saturday:

…to staring at this headline on Monday, and wondering, “What exactly is the FDA thinking???”

To be clear, I don’t have a problem with the Novavax vaccine in general. I get the appeal of a more standard Covid-19 vaccine, given the amount of fear-mongering around the mRNA vaccines, and the dismal uptake of the similarly novel J&J adenovirus vector vaccine. Novavax uses a common vaccine technique of incorporating protein subunits of the SARS-CoV-2 virus — i.e., no invasion of the cells by re-engineered adenovirus or microscopic bundles of mRNA — and increasing the immune response via an adjuvant. In this case, the adjuvant, Matrix-M, is derived from the Chilean soapbark tree, akin to the adjuvant used in the highly effective (and highly reactogenic) Shingrix vaccine against shingles.
That said, this is an EMERGENCY Use Authorization. Is Covid-19 still an emergency for teenagers, nearly 75% of whom already had antibodies to SARS-CoV-2 back in February, and who have had access to Pfizer’s vaccine for over a year? Below is the FDA’s criteria for an EUA:
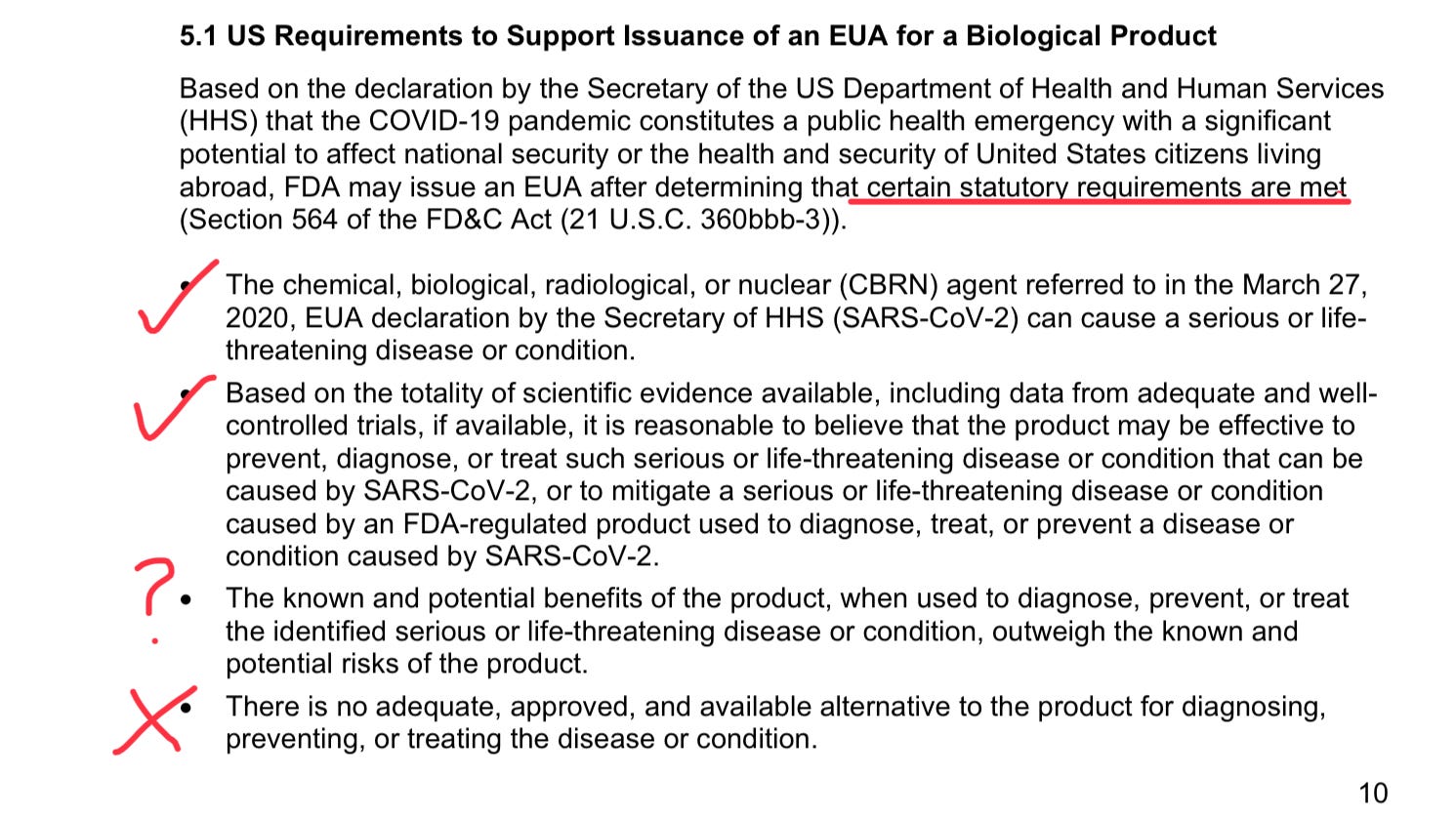
Some would quibble with my check marks on the first two requirements, but about 1 in 1500 teenagers have been hospitalized with Covid-19 per year during the pandemic, and the 80% Novavax vaccine efficacy in this age group (granted, in the pre-Omicron era, and among kids without prior infection) suggests protective benefit. However, how on earth do we define the Pfizer vaccine for 12-15 and 16 and up, and the Moderna vaccine for 12-17 year olds, if not “adequate, approved, and available” alternatives? Dr Peter Marks, head of the FDA’s Center for Biologics Evaluation and Research, unconvincingly parried these concerns by claiming that the more traditional nature of Novavax would make it substantially more appealing to the vaccine-hesitant. Most importantly, though, the FDA appears to have given little thought to the possibility that nearly half of the target population for their EUA might actually experience more risks than benefit by taking the Novavax vaccine. Allow me to explain.
Our data is a bit limited here, since the randomized controlled trials from Novavax have not been published, and the FDA decided to announce its approval in the unusual manner of not convening its Vaccines and Related Biologics Advisory Committee (“VRBAC”) first to tender a recommendation. All we have are the VRBAC meeting documents and the CDC ACIP slides for their June 2022 consideration of the Novavax product for adults, and the FDA Fact Sheet published upon granting the EUA for ages 12-17 last week.
What they show is yet another Covid vaccine with an alarming rate of vaccine-induced myocarditis in the cohort of young males. Somehow this was missed in some of the reporting of the initial Novavax EUA:
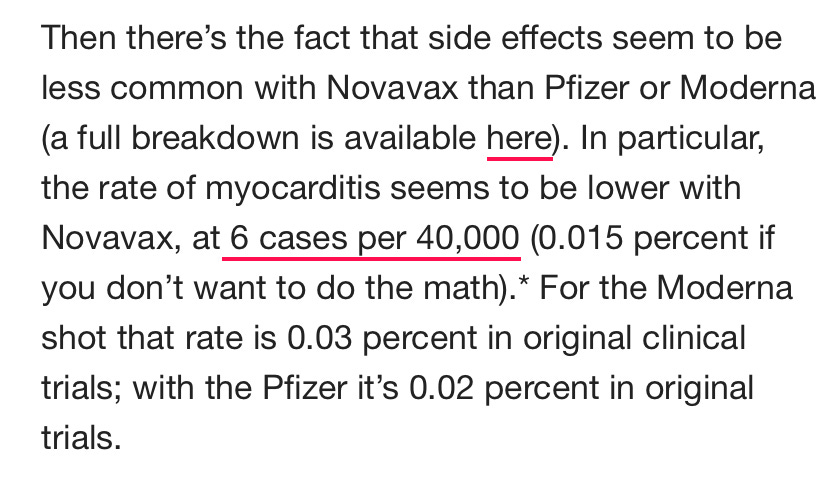
I did write the author to let her know that the myocarditis rate in the “original trials” for the 50,000 recipients of the Pfizer and Moderna vaccines was exactly zero. That is my concern with Novavax. They ended up administering at least one vaccine shot to about 42,000 participants, and described 4 clear cases of post-vaccine myocarditis or pericarditis. Again: none in the original 50,000-strong mRNA trials; 4 among the Novavax 42,000.
As most everyone knows by now, myocarditis is the predominant vaccine-related concern among teenage boys, with studies finding rates as high as 1 in 2700 with the Pfizer vaccine, and even greater frequency with Moderna and its higher dose. What might it be with Novavax?
Their original Study 301 included a little over 10,000 men over 17, and added about 1,100 more boys in the 12-17 range. They added about 10,000 booster recipients in another arm of Study 301. Additional adult studies in the UK (Study 302), South Africa (303) and Australia (304) added roughly another 8,000 men. With a median age of the adult Study 301 of 47, we would approximate (neither Novavax or the FDA provide us the exact numbers, unfortunately) that around 2,5000 men in the original study were under 30, plus the 1,100 boys 12-17. We can estimate about 1,100 men under 30 received the booster in Study 301 and another 1,700 from Studies 302-304. In that total cohort of some nearly 6,400 young men, we saw 3 clear-cut cases of post-vaccine myocarditis, per the VRBAC notes:
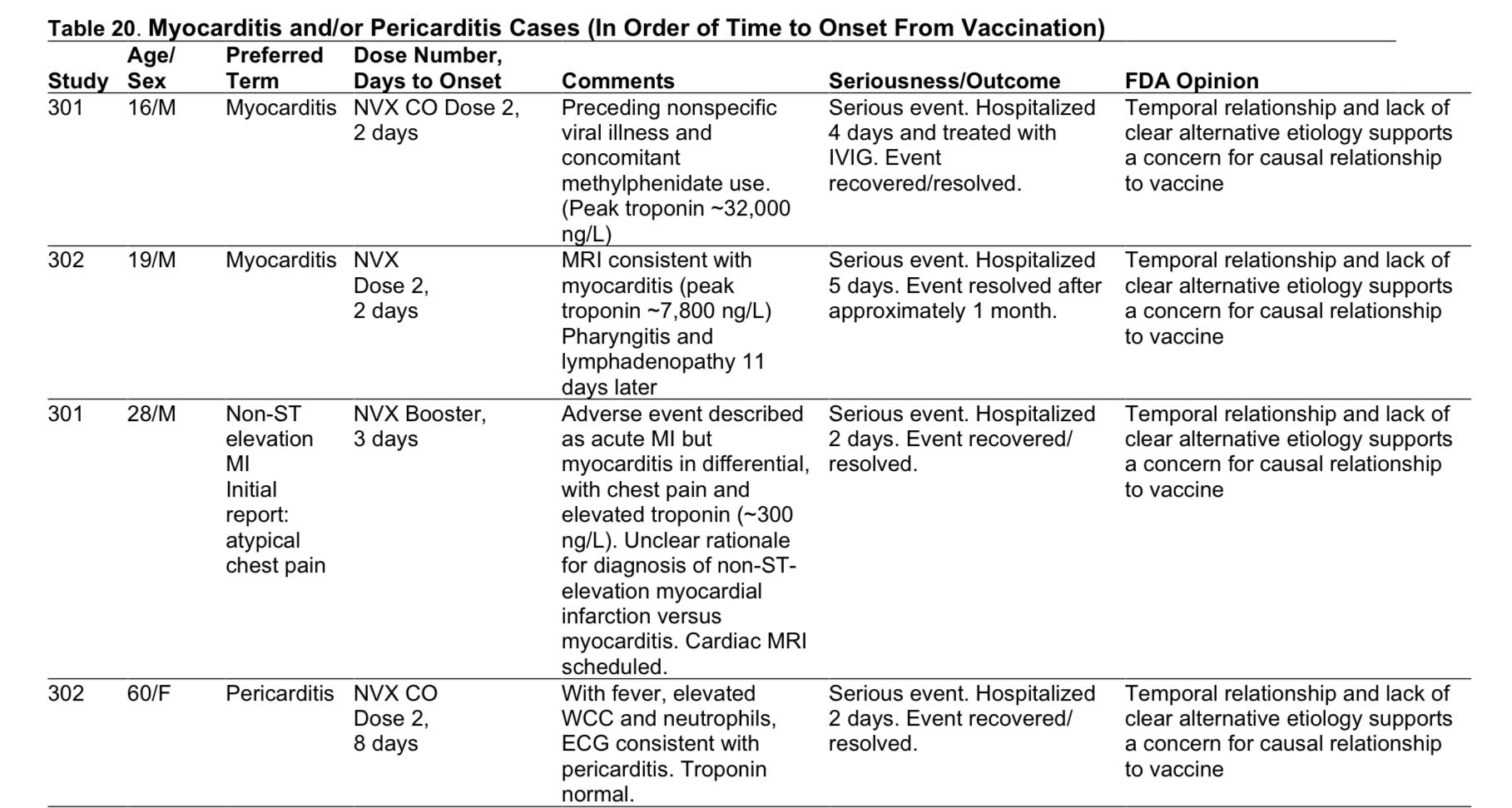
Now, I am not going to pretend that 3 in 6,400 is a hard number here. The sample size is too small to draw any conclusion other than, “this looks like a real problem.” Compounding the difficulties in assessing the risk, the smaller trials literally were done with a different manufacturing process, so we are told we cannot compare to the original trial data (!). I don’t find that terribly reassuring, especially considering that both earlier and later trials found myocarditis; and that I am not even considering the 4th case (of pericarditis) in a 60-year-old woman, and another case of myocarditis of questionable causation in a 20-year-old man. My best guess would be that the rate of post-vaccine myocarditis in young men will prove to be even higher than with the mRNA vaccines, or at least Pfizer; but it’s impossible to know with any certainty based on the data we have in hand.
It’s also impossible to deem, as the FDA did, that the risk of hospitalization after Novavax (from post-vaccine myocarditis alone) in a 12-17 year old male might not exceed the hospitalization risk from the virus itself. Recall that about 1 in 1500 teens have been hospitalized with Covid annually, whether for pneumonia, myocarditis, organ failure, or perhaps something unrelated to their viral infection, like a skin infection or broken bone that happened to align with a positive Covid test. For the probably 80-90% of teens who have already had Covid-19, the risk of severe disease should be at least 2-3X lower than that 1 in 1500 figure, especially if they lack risk factors like obesity or diabetes.
Then there are a multitude of unknowns, like how far that 80% efficacy will plummet with Omicron; if Novavax adds any protection to those with prior infection; whether Novavax will substantially reduce long Covid rates in “breakthrough” cases; and if the duration of protection against infection will last more than the few months studied.
My risk:benefit calculator informs me that, most likely, for a healthy 12-17 year old boy, certainly one with a prior Covid infection, their risk of a bad outcome is higher if they opt for 2 shots of Novavax than if they do not. I don’t think any re-tweaking of my numbers can lead to the opposite conclusion, at least with any certainty.
So why on earth is Peter Marks and the FDA ushering Novavax through in this low risk age group via an Emergency Use Authorization without even convening a VRBAC meeting? I am unsure how many vaccine-hesitant high risk teenagers without prior infection are left in the U.S., just waiting for Novavax to finally take the leap to vaccinate. I am guessing that number is tiny, and uptake figures will reveal that soon enough. If, on the other hand, enough teenage boys opt for the Novavax vaccine, post-marketing data might end up informing us that the rate of serious adverse events truly was unacceptable. Further putting at risk the plummeting credibility of the FDA for a marginally-useful vaccine product seems like another poor risk:benefit calculation.
As to why this keeps happening, many have written about the revolving door between Big Pharma and the FDA, ostensibly intended to regulate the pharmaceutical industry. Peter Marks, now leading these FDA meetings on authorizing Covid vaccines, worked on drug development for Genzyme and Novartis earlier in his career, and helped start up “Operation Warp Speed” as a partnership between vaccine makers and government. I don’t doubt that Dr Marks is a keen and experienced voice in any discussion about the value of a novel vaccine; but I do think it’s hard to let go of a desire to facilitate success for industry when that’s a major part of your professional background. It’s understandable. It’s also unacceptable, given that his role in the FDA is protecting the public health.
The FDA must be led by people who will make life uncomfortable for the Pharmaceutical Industry, especially when they bring products up for approval with shoddy trial data which cannot show clear evidence of benefit. Back in August 2020, Dr Marks made this promise:

Well, it’s time, Dr Marks. Thank you for your service, but it’s time to move on to greener pastures. I’ll send you the trail map.

Would you mind expanding on the "1 in 1500 teenagers have been hospitalized with Covid-19 per year during the pandemic" statement, Doctor? Am I reading it incorrectly, or misinterpreting it?
I was under the impression that it was approximately 1 in 48,000. Putting aside the "with or from" controversy, I understood adolescent hospitalizations had peaked at about a year into the epidemic. Here's where I read that statistic:
https://www.cdc.gov/mmwr/volumes/70/wr/mm7023e1.htm
From the above reference:
"COVID-19 adolescent hospitalization rates from COVID-NET peaked at 2.1 per 100,000 in early January 2021, declined to 0.6 in mid-March, and rose to 1.3 in April."
What am I misunderstanding?
Given hospitalisation is no longer the concerning metric, as significant data emerges for post covid sequela, long covid, and immune system depression, how would your risk assessment change taking into account these factors?